

source : the age
Jane Halton was in the room with the world’s top health chiefs as the World Health Organisation rang its most serious alarm about the Ebola outbreak.
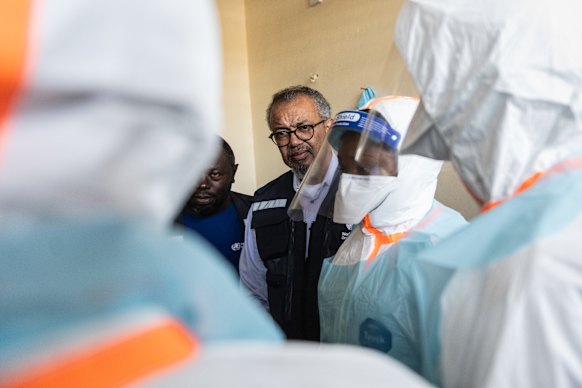
Those gathered on the sidelines of the World Health Assembly in Geneva included WHO’s director-general, Dr Tedros Adhanom Ghebreyesus, who had just declared the spreading sickness in the Democratic Republic of the Congo a public health emergency of international concern.
His phone kept buzzing.
“Terribly, in the course of that meeting, Tedros was getting text messages from WHO people on the ground who were actually being fired on in their tent,” Halton recalled of the May meeting. “It’s a very dangerous part of the world.”
Halton ran the Australian Health Department as secretary between 2002 and 2014, and was enmeshed with Australia’s pandemic response while serving on the National COVID-19 Co-ordination Commission.
Her remit expanded worldwide when she became chair of the Coalition for Epidemic Preparedness Innovations (CEPI). It’s a pandemic-busting alliance of government bodies, scientific outfits and civil organisations formed in the aftermath of the largest ever Ebola outbreak, which began in 2014. The viral haemorrhagic fever then infected 28,600 people and killed 11,325 across West Africa.



The current outbreak, some experts fear, could rival that disaster. There have been 569 confirmed cases and 103 deaths as of June 7 across the DRC and Uganda. Modelling shows that the actual case number could be double that. WHO chief Tedros warned last week that the disease may have festered for four months, spreading through bodily fluids including blood, vomit and semen, before the outbreak was announced on May 15.
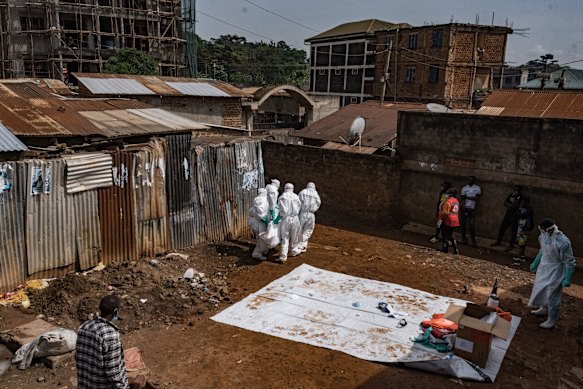
The region was ambushed by a rare strain of the Bundibugyo virus with no vaccine or treatment. Amid it all, bullets fly between warring militias, and misinformation adds to the violence. Medical tents have been torched by grieving family members of the dead who do not believe the virus killed their loved ones.
Last week, a group of young men stormed a hospital in eastern Congo to seize the bodies of two relatives. During the chaos, CNN reported, 18 suspected Ebola patients left the facility and disappeared.
These are nightmare conditions for disease containment. But CEPI has just poured $87 million into three possible weapons against the disease – a shot in the arm for three Bundibugyo vaccine candidates in early stages of development.
It’s a scattergun strategy that paid dividends during the last pandemic. “During COVID, CEPI had investments in 14 vaccine candidates, of which seven got to some form of licensure,” Halton says. “I describe this as the ‘many shots on goal’ approach.”


CEPI has become a cornerstone of the world’s response to deadly new pathogens. The non-profit foundation, partly funded by Australia, finances science aimed at crafting new countermeasures to emerging diseases in a pandemic-prone world.
It also runs disease control war games with laboratories and governments. In one such exercise, for example, it set a University of Queensland lab the challenge of crafting a vaccine for a bloody, deadly virus spread by the pygmy rice rat in 150 days.
There was no actual outbreak to address, but the hypothetical challenge was aimed at honing the world’s ability to rapidly craft new vaccines. Some practice drills, however, have proved eerily prescient.
CEPI ran an exercise involving the Rwandan government in September 2024. It laid out a fictional scenario of a young abattoir worker who falls sick with fever, joint pain and headaches. Three of his healthcare workers become infected with the mystery illness, and one dies. How should the government respond?
For this scenario, it was decided last minute that the disease should be Marburg, a haemorrhagic fever. The exercise helped health authorities to iron out their outbreak response plan and identify bottlenecks that could strangle rapid disease control.


Little did they know, at the same time, a real 27-year-old Rwandan miner had sickened with aches and fever. His pregnant wife fell ill too, as well as health workers at the hospital they attended. It was Marburg, flaring in Rwanda for the first time.
Match-fit from their war-game exercise, the government leapt into action, launching contact tracing and door-to-door surveillance while calling in CEPI and its partners to find a vaccine candidate. Rwanda had an emergency vaccine trial under way within 10 days of the outbreak, and the disease was controlled by December that year.
“One of the things we’ve learnt is how to move quickly, very quickly, through all the steps necessary to go from a possible candidate through to manufacturing,” Halton says.
Instead of basic science, animal work, human trials, peer review, regulatory applications and vaccine manufacturing happening one after the other, CEPI is facilitating ways to overlap these stages, streamlining the process so that if a vaccine succeeds, it can be released as soon as possible.



“If you do all of that in parallel, you shrink the time very significantly. CEPI has an understanding of all of this ecosystem, everything from the bench science all the way through to how you get a product produced and moved into a country,” Halton says.
“It’s getting rid of what I describe as the ‘white space’ in the timetable. There are no corners cut – it’s scientifically robust,” Halton says. But the approach does risk burning cash if a candidate falls over.
“If you want to save money, you spread everything out, you do it one at a time, and you don’t invest more money until the answer is very clear. But that takes a long time. We want access, and we want speed,” she says.
“If it costs more money, we don’t care – well, we do care, but we think that that is a premium the world should pay to actually get something that works.”
The world has no answer to Bundibugyo, even though it is so deadly and devastating, partly because it is too rare to guarantee market return for developers. That’s why CEPI has committed $87 million in “push” funding to get new vaccine candidates tested.
Meanwhile, Gavi, the Vaccine Alliance, has cleared $US40 million ($57 million) in “pull” funding to build production capability even before a vaccine is guaranteed to work. The “push-pull” strategy is designed to smooth the financial risks that developers take on by testing new vaccines, while ensuring safe and effective treatments get to the front lines as soon as possible.
CEPI has tipped $US50 million into preclinical testing and clinical trials for a Moderna Bundibugyo ebolavirus vaccine candidate, while manufacturing enough doses so that large-scale phase 2 and 3 trials can launch immediately if phase 1 succeeds.


$US3.2 million has gone to an IAVI candidate designed to trigger rapid-onset immunity. CEPI is also fast-tracking a third vaccine option with $US8.6 million based on the University of Oxford’s ChAdOx1 platform.
This method harnesses a weakened virus that causes the common cold in chimpanzees to deliver small, harmless fragments of another disease – in this case, Bundibugyo ebolavirus – and spark immunity. The platform was used in the AstraZeneca COVID-19 vaccine delivered 3 billion times during the COVID pandemic. WHO hopes human trials for the Ebola version could be under way in two to three months.

Halton is advocating for $US2.5 billion in funding for CEPI 3.0, a five-year pandemic preparedness plan aimed at making treatments to combat entire viral families rather than individual pathogens. Before the next globe-crippling illness – “disease X” – strikes, CEPI wants the world able to craft and distribute new vaccines within 100 days. That kind of speed would have saved about 8 million lives during the COVID-19 pandemic.
“It’s about speed, safety and scale to save lives,” Halton says. “That’s what we’re trying to do.”
The Examine newsletter explains and analyses science with a rigorous focus on the evidence. Sign up to get it each week.





