

Source : the age
By Pramudie Gunaratne
It’s 3am, and I’m sitting on the floor in a dark hospital corridor.
The pager clipped to the pocket of my scrubs is beeping again, and I am the only psychiatric doctor covering the hospital on the night shift. I was just called to the mental health ward where a 19-year-old girl, tormented by voices, was banging her head on the bed rails.
Dr Pramudie Gunaratne: NSW is the state with the lowest per capita spending on mental health.Credit: Louise Kennerley
Nurses had transferred her to the “seclusion room”, and from the small window cut out of the door I could see her whispering to herself as she lay curled on the single blue mattress on the floor. I wish we had another way to keep her safe overnight.
There are patients still queued in the emergency department waiting to see me: a university student slumped in a chair with a blanket over her shoulders after an ambulance had brought her in from the edge of a nearby cliff top, a young man with bloodshot eyes pacing barefoot flanked by two security guards after police found him wandering through traffic, a 12-year-old girl with bandaged wrists and her parents in tears. This is not an extraordinary shift. Any psychiatrist or trainee could tell you that this is the story of every night in hospitals across our state.
It is an incredible privilege to be given the responsibility of caring for people when they are at their most vulnerable. Yet, as doctors, we need to work within a system that allows us to provide that care.
In NSW, our public mental health system has been running (or more accurately, limping) with 30 per cent of psychiatrist positions unfilled. Even in the most prestigious hospitals in central Sydney, vacancies for psychiatrists have become abundant.
The caseloads for individual doctors are extreme. The injustice of sending patients away from our overloaded services when they are desperate for help weighs heavily. Even when people are accepted into care, the system is so under-resourced that clinicians cannot provide the standard of care that they are trained to give. This is why I needed to leave a broken system, before it broke me.
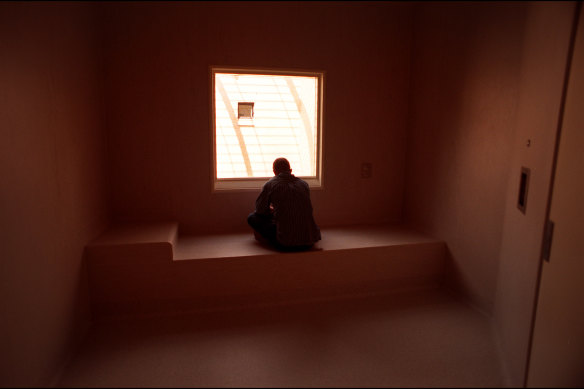
A seclusion room is used for the sole confinement of a distressed or agitated person.Credit: Eamon Gallagher
The current situation is unsurprising given NSW is the state with the lowest per capita spending on mental health. We are also bleeding psychiatrists across the borders given the significant pay gap for public psychiatrists compared with our neighbouring states. Disappointingly, 15 months of discussions with the state government regarding this chronic understaffing and under-resourcing has resulted in little action. Now, 203 of the state’s remaining 295 public psychiatrists have submitted their resignations and are preparing to walk.
This mass exodus has been described as a “pay dispute”, but the truth is that there is no shortage of work in psychiatry. If these psychiatrists were simply interested in increasing their income, there are myriad options available to them. These doctors could easily step into the private sector, take a locum position in their own hospital or move interstate.
Instead, public psychiatrists choose this work so they can care for some of the most marginalised people in our society and for people with the most severe and chronic mental illnesses. These psychiatrists are resigning in despair. They can no longer provide the care their patients need, and the future of public mental health care in NSW is under threat as the working conditions and uncompetitive remuneration make it impossible to recruit junior psychiatrists.
The state government says it cannot afford to improve remuneration. However, the government’s own data shows there has been a threefold increase in the use of “locum” or temporary psychiatrists over the past two years to plug holes and keep services barely afloat. These temporary psychiatrists are paid two to three times the pay rates of permanent psychiatrists.
If more competitive remuneration could bring permanent psychiatrists back to even a fraction of the unfilled positions at present, it would significantly reduce expenditure on locum psychiatrists and save taxpayer dollars. This is not even counting the savings that flow from more effective patient care by permanent psychiatrists who know their patients and are invested in improving local services.
Of course, our government is well aware of this simple cost calculation. Any punter at the pub can understand that if you improve conditions for permanent staff, you will need fewer temporary staff. So, perhaps the challenge is not about the dollars – instead, it is the politics of being seen to increase remuneration in mental health while strikes continue in other areas.
However, we need our leaders to stop playing politics. They need to have the courage to start fixing a broken system before there is no system left at all. The proposal to waste even more taxpayer dollars on locum psychiatrists may help the government save face in the short term, but it does nothing to save lives. Instead, it will likely cause more harm.
Dr Pramudie Gunaratne is a psychiatrist based in Sydney.





